




郝晓军 校译
Valsalva视网膜病变在眼科论著中罕有报道,今天学习的是wills眼科著作中关于此病的描述,明天本公众号将继续推出尖峰微信群内关于该病变治疗的讨论内容。
第二十一节 Valsalva视网膜病变
【症状】
视力下降,或无症状。Valsalva动作史(声门关闭,猛力呼气),可出现在提起重物、咳嗽、呕吐、便秘时用力。有时无Valsalva动作史可循。
【体征】
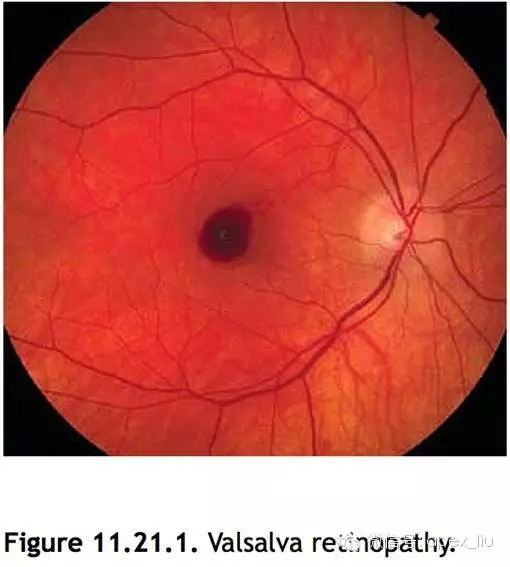
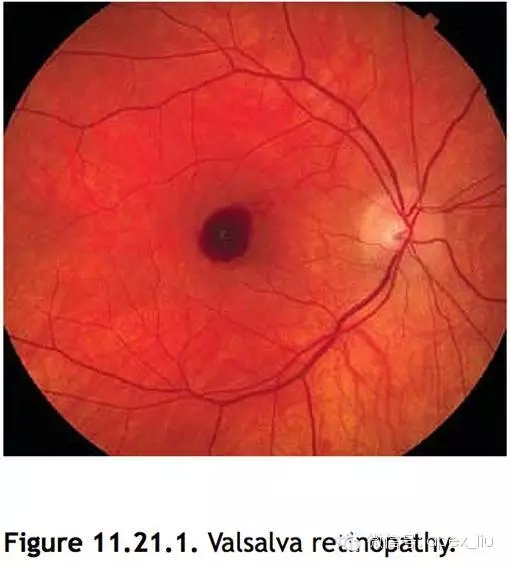
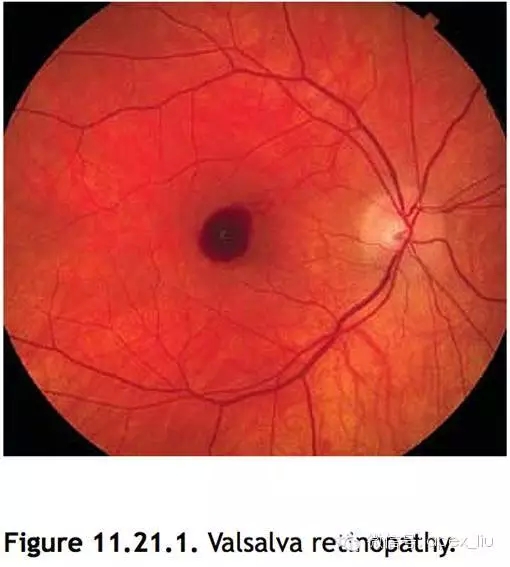
见图11.21.1。
【主要体征】
黄斑区内界膜(ILM)下方一处或多处出血。单眼发病或双眼。数天后出血转变为黄色。
【其他体征】
玻璃体和视网膜下出血,以及球结膜下出血。
【鉴别诊断】
1、玻璃体后脱离 可造成玻璃体急性出血,以及周边视网膜和视盘边缘出血。通常无内界膜下出血。参见本章节玻璃体后脱离。
2、视网膜大动脉瘤 多层视网膜出血,玻璃体出血,硬性渗出呈环状包绕着大动脉瘤。
3、糖尿病性视网膜病变 双眼的微血管瘤、点片状出血和硬性渗出。无单纯的内界膜下出血。可造成玻璃体出血。参见本章第十二节糖尿病性视网膜病变。
4、视网膜中央静脉阻塞或视网膜分支静脉阻塞 单眼发病,多发的视网膜内出血,静脉扩张迂曲。参见本章第八节视网膜中央静脉阻塞和第九节视网膜分支静脉阻塞。
5、贫血或白血病 双侧的多发性火焰状和点片状出血,棉绒斑。也可出现内界膜下出血。
6、视网膜撕裂伤 撕裂伤可被出血包绕,变得模糊不清。撕裂伤很少出现在黄斑区。
【病因学】
Valsava动作使眼内静脉压的突然升高,造成黄斑区浅表的毛细血管破裂。可与抗凝治疗有关。
【检查】
1、病史 近期有无Valsalva动作史,包括提起重物、便秘时用力、咳嗽、喷嚏、呕吐等?患者可不记得有过Valsalva动作。
2、全面的眼科检查 包括使用裂隙灯联合60D或90D透镜和间接检眼镜散瞳检查眼底。寻找支持其他致病原因的体征。包括微血管瘤、点片状出血、棉绒斑、视网膜撕裂伤、玻璃体后脱离。
3、如果玻璃体积血浓厚,需行眼科B超 以排除视网膜撕裂伤。
4、眼底荧光血管造影 可用于排除其他致病原因,包括视网膜大动脉瘤和糖尿病性视网膜病变。
【治疗】
1、预后非常好。大部分患者仅需观察,内界膜下出血于数天至数周后吸收。
2、偶有激光使积血引流至玻璃体,使黄斑暴露出来。
3、很偶尔使用玻璃体切除清除玻璃体积血。
【随访】
初诊的患者每隔2周复诊1次,监测积血吸收情况,然后常规复诊。
11.21 Valsalva Retinopathy
Symptoms
Decreased vision or asymptomatic. History of Valsalva maneuver (forceful exhalation against a closed glottis), which may occur during heavy lifting, coughing, vomiting, constipation, straining. Sometimes no history of Valsalva can be elicited.
Signs
(See Figure 11.21.1.)
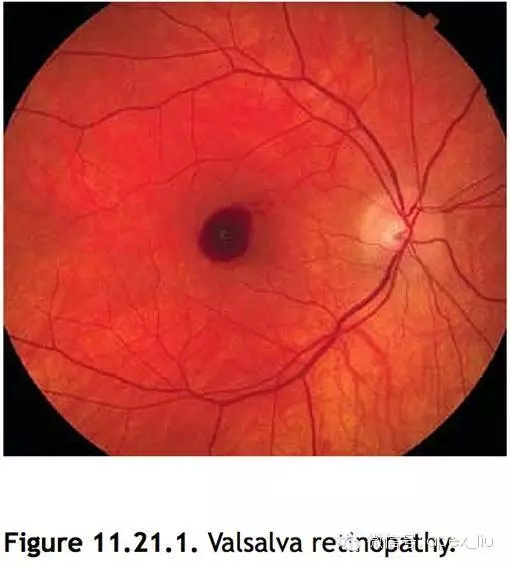
Critical. Single or multiple hemorrhage(s) under the internal limiting membrane (ILM) in the area of the macula. Can be unilateral or bilateral. Blood may turn yellow after a few days.
Other. Vitreous and subretinal hemorrhage can occur, as well as subconjunctival hemorrhage.
Differential Diagnosis
(1)Posterior vitreous detachment: Can cause vitreous hemorrhage acutely as well as peripheral retinal and disc margin hemorrhages. However, typically no sub-ILM hemorrhage. See 11.1, Posterior Vitreous Detachment.
(2)Retinal arterial macroaneurysm: Hemorrhages in multiple layers of the retina and vitreous hemorrhage. Can also have a circinate ring of hard exudates around a macroaneurysm. See 11.19, Retinal Arterial Macroaneurysm.
(3)Diabetic retinopathy: Microaneurysms, dot-blot hemorrhages and hard exudates bilaterally, not isolated sub-ILM hemorrhage. Both can cause vitreous hemorrhage. See 11.12, Diabetic Retinopathy.
(4)CRVO or BRVO: Unilateral, multiple intraretinal hemorrhages, venous dilation, and tortuosity. See 11.8, Central Retinal Vein Occlusion, and 11.9, Branch Retinal Vein Occlusion.
(5)Anemia or leukemia: May have multiple, bilateral flame and dot-blot hemorrhages as well as cotton–wool spots. Can also present with sub-ILM hemorrhage.
(6)Retinal tear: Can be surrounded by hemorrhage obscuring the tear. Tears rarely occur in the macula.
Etiology
Valsalva causes sudden increase in intraocular venous pressure leading to rupture of superficial capillaries in macula. May be associated with anticoagulant therapy.
Work-Up
(1)History: History of Valsalva including any recent heavy lifting, straining while constipated, coughing, sneezing, vomiting, etc? The patient may not remember the incident.
(2)Complete ocular examination, including dilated retinal examination with a slit lamp and a 60- or 90-diopter lens, and indirect ophthalmoscopy. Look for findings suggestive of a different etiology including microaneurysms, dot-blot hemorrhages, cotton– wool spots, retinal tear, PVD.
(3)If dense vitreous hemorrhage is present, then obtain B-scan US to rule out a retinal tear.
(4)IVFA may be helpful to rule out other causes including retinal arterial macroaneurysm or diabetic retinopathy.
Treatment
Prognosis is excellent. Most patients are observed as usually sub-ILM hemorrhage resolves after a few days to weeks. Occasionally laser is used to permit the blood to drain into the vitreous cavity thereby uncovering the macula. Vitrectomy rarely considered for nonclearing vitreous hemorrhage.
Follow-Up
May follow-up every 2 weeks for the initial visits to monitor for resolution, then follow-up routinely.















信息提要:眼科医院 激光近视手术 飞秒激光近视手术 近视手术价格 白内障手术 青光眼手术 斜弱视手术 黄斑病变治疗 角膜移植 视网膜脱落手术费用 预约挂号
南京医科大学眼科医院 @2013 - 2020 版权所有,网站备案号: 苏ICP备10209536号-1 ![]() 公安联网备案号:32010602010072
公安联网备案号:32010602010072
友情提示:本网站信息仅作健康参考,不作为医疗诊断和治疗依据,具体诊疗请遵照医师意见
汉中路院区地址:南京市鼓楼区汉中路138号 咨询电话(工作时间接听):025-86677777 025-86677702 药研机构:025-86677717
六合院区地址:南京市六合区雄州东路101号 咨询电话:025-57136532(工作时间接听)
工作时间:上午8:00--12:00 下午:13:30--17:00 (秋冬),14:00--17:30 (春夏)


